What is cholesterol?
There are few villains in the diet and health space with a worse reputation than cholesterol. How has cholesterol become so demonised and does it deserve the bad press it receives?
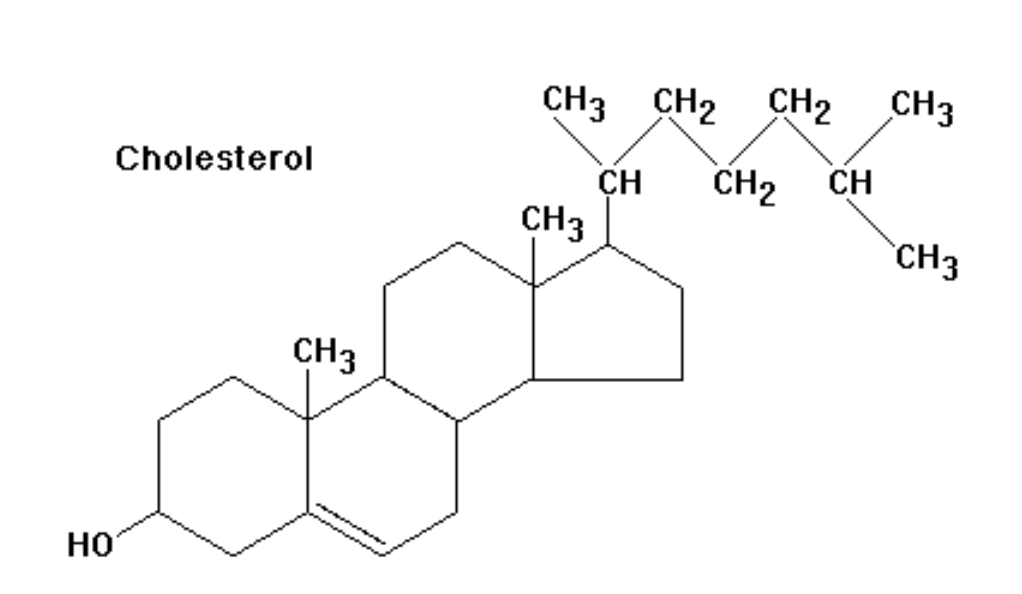
First let’s get this important point out of the way – cholesterol is essential to life. So if your goal is to rid your body of cholesterol, that may not end so well!
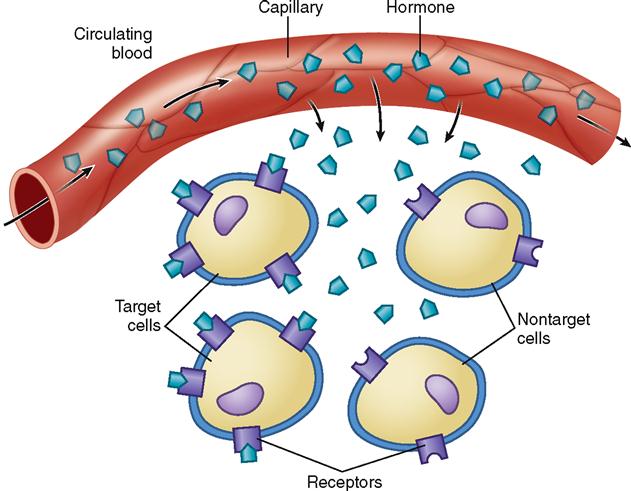
Cholesterol is vital to human survival as it is the primary component of the cell membrane of every cell in your body. Secondly it is the base or foundational building block of all the steroid hormones in our body – hello cortisol, progesterone, DHEA, testosterone, and estrogen!
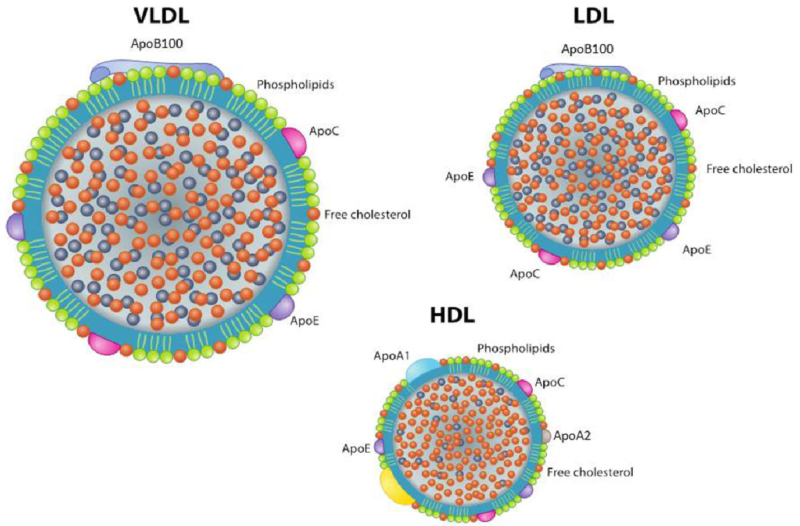
We broadly speak of cholesterol in two categories: Low Density Lipoprotein Cholesterol (LDL) and High Density Lipoprotein Cholesterol (HDL) and they have different jobs.
For simplicity sake we need to understand a couple of points:
-
LDL cholesterol particles are larger and less dense; they start in the liver and deliver the necessary cholesterol out to the rest of the body.
-
HDL, is much smaller and heavier; it transports excess cholesterol from the body, back to the liver for removal.
Given the very important role of cholesterol to the structure and functioning of our bodies, both of these forms of lipoproteins are GOOD.
So why the bad rap?
Well, when certain particles of a certain size and density bang into the sides of our blood vessels and arteries, they damage the cells lining the walls of the vessels (this lining is known as the endothelium), become embedded, inflamed, then calcified, and ultimately cause the narrowing of the passage in which blood can flow, leading to cardiovascular disease, heart attacks, and strokes.
If you guessed this evil, damage-causing culprit to be LDL, you would be (mostly) correct. Why only mostly correct ?
Well, what we measure when we measure LDL-c is how much cholesterol (shown by the orange dots above) is carried within the lipoprotein (a carrier molecule made of protein on the outside so that lipids, which are not water soluble, can move around in plasma or blood).
Does it actually matter how much of that cholesterol is contained within the lipoprotein? Not so much.
What does matter? The number of particles and the size of the particles. Think of a roadway – the likelihood of vehicles being in an accident – hitting each other or running into the guard rails (ie the endothelium), in a confined space has more to do with the size and number of vehicles, NOT how many passengers are in the vehicles. Ultimately if you want more meaningful information you should really be testing your Apo-A (corresponds to HDL) and Apo-B (corresponds to LDL) in addition to the standard lipid measurements of cholesterol, as they are more indicative of the particle number.
The next important point to make is that the vast majority (+80% of your body’s cholesterol) is endogenous – that means it is made by your body. A VERY small percentage of your cholesterol comes from the food you eat! Most dietary cholesterol is in the wrong form, and is unusable by the body unless it undergoes a chemical reaction. Who knew right? So much for the anti -egg crusade!